MEDICAL REFRACTORY EPILEPSY
PROCEDURES
VNS, vagus nerve stimulation
The procedure involves implanting a generator and vagus nerve stimulation electrodes under the skin. The procedure is performed without age restrictions. The antiepileptic mechanism of vagus nerve stimulation is not fully understood. The effect of stimulation of vagus nerve structures (myelinated and nonmyelinated fibers) is believed to be directly on the nucleus of the solitary band, and from there toward the limbic system and the insula.

VNS SenTiva Stimulator
SenTiva is an implantable and programmable pulse generator for the treatment of refractory epilepsy. It provides stimulation that responds to the rapid increase in heart rate that can be associated with seizures, allows day-night programming, schedule programming, and logging of low heart rate events and abdominal position.
DBS, deep brain stimulation
A novel method, it involves stereotactic implantation bilaterally into the deep structures of the brain of a small electrode connected to a stimulator placed under the skin or pectoral muscle. The stimulators record a recording of the brain’s bioelectrical activity and respond only if abnormal discharges occur. During DBS, stimulation can target one or multiple epileptic foci. Stimulation of the deep nuclei results in secondary diffuse stimulation of extensive cortical areas by taking advantage of the many pathways and connections that exist between deep structures and areas of the cortex.
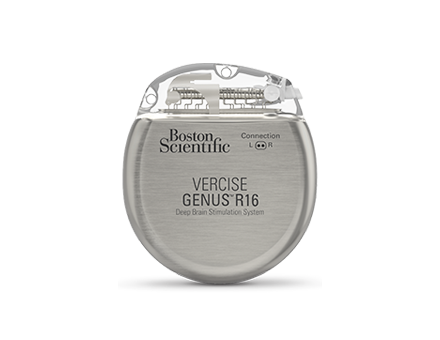
For neurostimulation of deep brain structures, we use Boston Scientific’s Vercise Genus rechargeable stimulator:
The Vercise Genus R16 stimulator is equipped with Cartesia 3D technology, a set of programming features that provide targeted therapy with less risk of side effects. It also makes it easier for the doctor to adjust and fine-tune the stimulation over time, so the patient can be sure to continue receiving the therapy they need. Because the battery can be recharged wirelessly for at least 15 years, several non-rechargeable pacemaker replacement procedures can be avoided during that time.
Features of the stimulator:
– Light weight and size of the device, the patient experiences less discomfort after implantation
– Battery life of at least 15 years, covered by warranty
– Wireless battery charging
– Bluetooth wireless remote control
– MR examination capability
– Constant-current stimulators
– With Cartesia 3D technology, Vercise DBS electrodes allow independent control and precise adjustment of stimulation size and shape, accurately targeting therapy and avoiding unwanted side effects
As part of the lobectomy procedure, the part of the lobe of the brain that is responsible for generating epileptic seizures is removed. Most often, the medial structures of the temporal lobe are removed (amygdalohippocampectomy).
Intraoperative Neuromonitoring
Intraoperative neuromonitoring is a diagnostic tool that is used during surgery. This method is based on the fact that nerve impulses are in the form of microelectric impulses which can be detected with super-sensitive equipment. During surgery, impulses are detected and recorded from the cortex of the brain responsible for example for hand movement. This method is also used for intraoperative mapping of eloquent structures for example visual or speech cortex. In that case direct electrical stimulation is used to induce neurological effects (speech arrest, visual disturbances, etc.) during awake craniotomy. This method allows to increase safety and improves neurological outcome of neurosurgical procedures. Intraoperative neuromonitoring performed during deep brain stimulation surgery is necessary for correct electrode placement by the neurosurgeon.
Lesionectomy surgery focuses on removing an isolated lesion (such as a tumor or malformed blood vessel) that is responsible for epileptic seizures.
Intraoperative Neuromonitoring
Intraoperative neuromonitoring is a diagnostic tool that is used during surgery. This method is based on the fact that nerve impulses are in the form of microelectric impulses which can be detected with super-sensitive equipment. During surgery, impulses are detected and recorded from the cortex of the brain responsible for example for hand movement. This method is also used for intraoperative mapping of eloquent structures for example visual or speech cortex. In that case direct electrical stimulation is used to induce neurological effects (speech arrest, visual disturbances, etc.) during awake craniotomy. This method allows to increase safety and improves neurological outcome of neurosurgical procedures. Intraoperative neuromonitoring performed during deep brain stimulation surgery is necessary for correct electrode placement by the neurosurgeon.
The corpus callosum is a set of nerve fibers connecting the two halves of the brain. Cutting the fibers – a calozotomy is an operation in which all or part of this structure is cut, resulting in a lack of communication between the hemispheres and preventing seizures from spreading from one side of the brain to the other. The procedure is called a disconnection.
Intraoperative Neuromonitoring
Intraoperative neuromonitoring is a diagnostic tool that is used during surgery. This method is based on the fact that nerve impulses are in the form of microelectric impulses which can be detected with super-sensitive equipment. During surgery, impulses are detected and recorded from the cortex of the brain responsible for example for hand movement. This method is also used for intraoperative mapping of eloquent structures for example visual or speech cortex. In that case direct electrical stimulation is used to induce neurological effects (speech arrest, visual disturbances, etc.) during awake craniotomy. This method allows to increase safety and improves neurological outcome of neurosurgical procedures. Intraoperative neuromonitoring performed during deep brain stimulation surgery is necessary for correct electrode placement by the neurosurgeon.
It is a type of hemispherectomy, a procedure that involves the resection of one hemisphere of the brain. Functional hemispherectomy is the separation of one hemisphere from the other and removal of a small part of the brain. It is used in situations where the entire hemisphere is not working properly.
Intraoperative Neuromonitoring
Intraoperative neuromonitoring is a diagnostic tool that is used during surgery. This method is based on the fact that nerve impulses are in the form of microelectric impulses which can be detected with super-sensitive equipment. During surgery, impulses are detected and recorded from the cortex of the brain responsible for example for hand movement. This method is also used for intraoperative mapping of eloquent structures for example visual or speech cortex. In that case direct electrical stimulation is used to induce neurological effects (speech arrest, visual disturbances, etc.) during awake craniotomy. This method allows to increase safety and improves neurological outcome of neurosurgical procedures. Intraoperative neuromonitoring performed during deep brain stimulation surgery is necessary for correct electrode placement by the neurosurgeon.
Morell’s procedure is used when epilepsy originates in areas that cannot be removed. The surgeon makes a series of incisions that interrupt the course of seizure impulses, but do not damage the brain.
Intraoperative Neuromonitoring
Intraoperative neuromonitoring is a diagnostic tool that is used during surgery. This method is based on the fact that nerve impulses are in the form of microelectric impulses which can be detected with super-sensitive equipment. During surgery, impulses are detected and recorded from the cortex of the brain responsible for example for hand movement. This method is also used for intraoperative mapping of eloquent structures for example visual or speech cortex. In that case direct electrical stimulation is used to induce neurological effects (speech arrest, visual disturbances, etc.) during awake craniotomy. This method allows to increase safety and improves neurological outcome of neurosurgical procedures. Intraoperative neuromonitoring performed during deep brain stimulation surgery is necessary for correct electrode placement by the neurosurgeon.
NEUROSURGERY DEPARTMENT
CONTACT
Vital Medic
46-200 Kluczbork
Skłodowskiej-Curie st. 21
Poland, opolskie region
Contact to our patient service:
📱 +48 531 999 172
📱 +48 531 439 671
✉ neuro@vitalmedic.pl
MAIN EMAIL
PATIENT COORDINATOR
Paweł Respondek
📞 +48 531 999 172
✉ p.respondek@vitalmedic.pl
PATIENT CARER
Nicoletta Nicowska
📞 +48 531 439 671
✉ n.nicowska@vitalmedic.pl
LEAVE US MESSAGE
WE WILL GET BACK TO YOU
PERSONNEL

Witold Libionka, MD PhD
specialist in neurosurgery and neurotraumatology

Anna Włodarczyk, Msc
psychologist, psychotherapist

Mateusz Pawłowski, MD
specialist in neurosurgery
